

What are EDS and HSD?
What is EDS?
The Ehlers-Danlos syndromes (EDS) are a group of 13 heritable connective tissue disorders. Each type of EDS has its own diagnostic criteria based on the set of symptoms and features observed in that type.
What is HSD?
The hypermobility spectrum disorders (HSD) are diagnosed when a person has symptomatic joint hypermobility that can’t be explained by other conditions, such as EDS.
EDS and HSD Diagnosis in Adults
Hypermobile Ehlers-Danlos Syndrome
Hypermobile EDS (hEDS) is the most common type of EDS. There is no genetic test for hEDS because the cause(s) of hEDS have not been identified.
hEDS is diagnosed when an adult meets the diagnostic criteria for hEDS.
Other Types of Ehlers-Danlos Syndrome
The other 12 types of EDS do have genetic tests available.
If a person meets the diagnostic criteria for one of these types of EDS, genetic testing is recommended to confirm the diagnosis.
Hypermobility Spectrum Disorders
The hypermobility spectrum disorders (HSD) are diagnosed based on:
- Medical history
- Physical examination
- Ruling out other conditions that can cause similar symptoms
EDS and HSD Diagnosis in Children
Hypermobility Spectrum Disorders
Children and adolescents from age 5 through biological maturity can be assessed for HSD using the 2023 Diagnostic Framework for Pediatric Joint Hypermobility.
When a person reaches biological maturity (at age 18 or the completion of bone growth), they may be reassessed using the diagnostic criteria for hEDS.
Ehlers-Danlos Syndromes
Though children cannot be diagnosed with hEDS, they can be assessed for the other types of EDS.
If a person meets the diagnostic criteria for one of these types of EDS, genetic testing is recommended to confirm the diagnosis.
Check out our Genetics and Inheritance page for more information about genetic testing.
Diagnostic Criteria
There is currently no laboratory test available to diagnose hEDS. The diagnosis of hEDS is given to adults who meet the clinical diagnostic criteria for hEDS. Children and adolescents with generalized joint hypermobility can be assessed using the pediatric diagnostic framework.
To meet the diagnostic criteria for hEDS, a person must meet all three criteria (1 and 2 and 3).
Criterion 1: Generalized joint hypermobility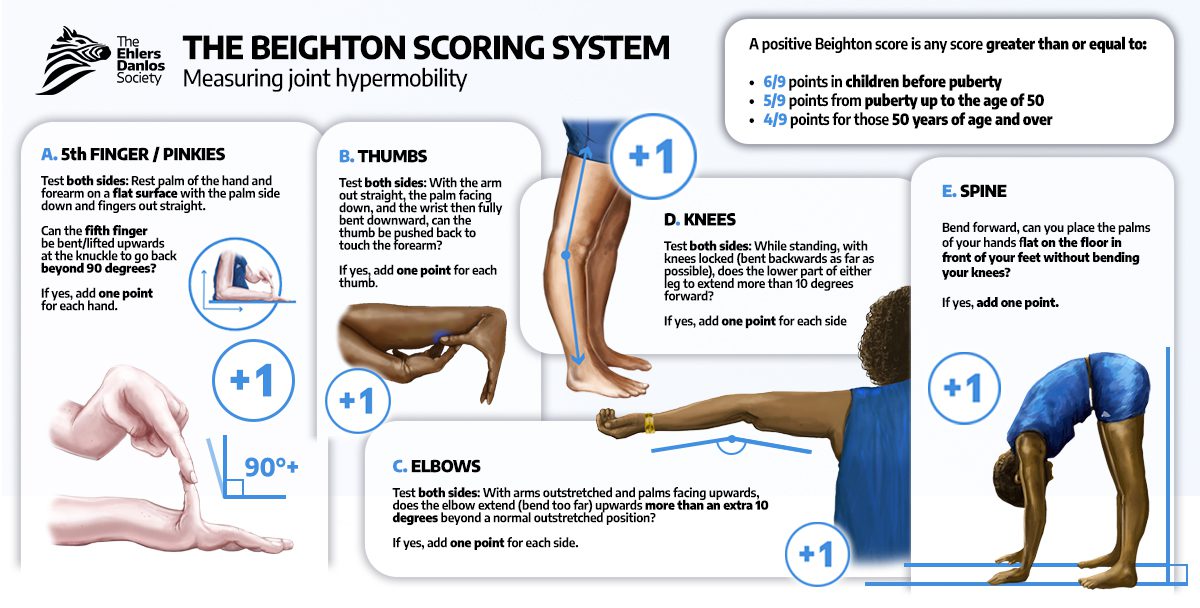
Criterion 2: Two or more of the following features (A, B, and C) must be presentFeature A: Manifestations of a connective tissue disorder (must have five or more of the following):
- Unusually soft or velvety skin
- Mild skin hyperextensibility
- Unexplained striae such as striae distensae or rubrae at the back, groins, thighs, breasts, and/or abdomen in adolescents, men, or pre-pubertal women without a history of significant gain or loss of body fat or weight
- Bilateral piezogenic papules of the heel
- Recurrent or multiple abdominal hernia(s) (e.g., umbilical, inguinal, crural)
- Atrophic scarring involving at least two (2) sites and without the formation of truly papyraceous and/or hemosideric scars as seen in classical EDS
- Pelvic floor, rectal, and/or uterine prolapse in children, men or nulliparous women without a history of morbid obesity or other known predisposing medical condition
- Dental crowding and high or narrow palate
- Arachnodactyly, as defined in one or more of the following:
- positive wrist sign (Steinberg sign) on both sides
- positive thumb sign (Walker sign) on both sides
- Arm span-to-height ratio ≥ 1.05
- Mitral valve prolapse (MVP) mild or greater based on strict echocardiographic criteria
- Aortic root dilatation with Z-score >+2
Feature B: Positive family history (one or more first-degree relatives independently meet the current diagnostic criteria for hEDS)
Feature C: Musculoskeletal complications (must have at least one of the following):
- Musculoskeletal pain in two or more limbs, recurring daily for at least three (3) months
- Chronic, widespread pain for at least three (3) months
- Recurrent joint dislocations or frank joint instability, in the absence of trauma (a or b)
- Three (3) or more atraumatic dislocations in the same joint or two (2) or more atraumatic dislocations in two (2) different joints occurring at different times
OR - Medical confirmation of joint instability at two (2) or more sites not related to trauma
- Three (3) or more atraumatic dislocations in the same joint or two (2) or more atraumatic dislocations in two (2) different joints occurring at different times
Criterion 3: ALL of the following prerequisites must be met:
- Absence of unusual skin fragility, which should prompt consideration of other types of EDS
- Exclusion of other heritable and acquired connective tissue disorders, including autoimmune rheumatologic conditions
- In patients with an acquired connective tissue disorder (e.g., lupus, rheumatoid arthritis, etc.), additional diagnosis of hEDS requires meeting both Features A and B of Criterion 2. Feature C of Criterion 2 (chronic pain and/or instability) cannot be counted towards a diagnosis of hEDS in this situation.
- Exclusion of alternative diagnoses that may also include joint hypermobility by means of hypotonia and/or connective tissue laxity. Alternative diagnoses and diagnostic categories include, but are not limited to:
- Neuromuscular disorders (such as myopathic EDS and Bethlem myopathy)
- Other heritable connective tissue disorders (such as other types of EDS, Loeys–Dietz syndrome, Marfan syndrome)
- Skeletal dysplasias (such as osteogenesis imperfecta)
HSD in Adults
Adults are diagnosed with HSD if they have symptomatic joint hypermobility that cannot be explained by other conditions. There are four types of HSD in adults based on the type of joint hypermobility present:
")
HSD in Children and Adolescents
Children and adolescents with generalized joint hypermobility can be assessed using the 2023 Diagnostic Framework for Pediatric Joint Hypermobility. Children with generalized joint hypermobility may fit into one of eight categories based on their symptoms.
Children and adolescents may also be diagnosed with localized HSD (L-HSD) or peripheral HSD (P-HSD) if they have joint hypermobility in specific areas rather than throughout the body. Once a child reaches biological maturity, they can be assessed using the diagnostic criteria for hEDS.
| Pediatric Generalized Joint Hypermobility [pGJH] Subtypes | Musculoskeletal Complications | Skin and Tissue Abnormalities | Core Comorbidities |
| Pediatric generalized joint hypermobility | Absent | Absent | Absent |
| Pediatric generalized joint hypermobility with skin involvement | Absent | Present | Absent |
| Pediatric generalized joint hypermobility with core comorbidities | Absent | Absent | Present |
| Pediatric generalized joint hypermobility with core comorbidities and with skin involvement | Absent | Present | Present |
| Pediatric Generalized Hypermobility Spectrum Disorder [pgHSD] Subtypes | Musculoskeletal Complications | Skin and Tissue Abnormalities | Core Comorbidities |
| Pediatric generalized hypermobility spectrum disorder, musculoskeletal subtype | Present | Absent | Absent |
| Pediatric generalized hypermobility spectrum disorder, musculoskeletal subtype with skin involvement | Present | Present | Absent |
| Pediatric generalized hypermobility spectrum disorder, systemic subtype | Present | Absent | Present |
| Pediatric generalized hypermobility spectrum disorder, systemic subtype with skin involvement | Present | Present | Present |

If a person meets the diagnostic criteria for cEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has a genetic variant that causes cEDS.
To meet the diagnostic criteria for cEDS, a person must meet:
- Major criterion 1 AND major criterion 2
OR - Major criterion 1 AND three or more minor criteria
Major Criteria
- Skin hyperextensibility and atrophic scarring
- Generalized joint hypermobility
Minor Criteria
- Easy bruising
- Soft, doughy skin
- Skin fragility (or traumatic splitting)
- Molluscoid pseudotumors
- Subcutaneous spheroids
- Hernia (or history thereof)
- Epicanthal folds
- Complications of joint hypermobility (e.g., sprains, dislocations/subluxations, pain, flexible flatfoot)
- Family history of a first-degree relative who meets clinical criteria
Genetic testing is used to see if a person has a genetic variant that causes vEDS. Genetic testing should be considered if a person has any of the major criteria or several minor criteria, particularly in people under the age of 40.
Major Criteria
- Family history of vEDS with a documented causative variant in COL3A1
- Arterial rupture at a young age
- Spontaneous sigmoid colon perforation in the absence of known diverticular disease or other bowel pathology
- Uterine rupture during the third trimester in the absence of previous C-section and/or severe peripartum perineum tears
- Carotid-cavernous sinus fistula (CCSF) formation in the absence of trauma
Minor Criteria
- Bruising unrelated to identified trauma and/or in unusual sites such as the cheeks and back
- Thin, translucent skin with increased venous visibility
- Characteristic facial appearance
- Spontaneous pneumothorax
- Acrogeria
- Talipes equinovarus
- Congenital hip dislocation
- Hypermobility of small joints
- Tendon and muscle rupture
- Keratoconus
- Gingival recession and gingival fragility
- Early-onset varicose veins (under age 30 and starting before pregnancy if female)
If a person meets the diagnostic criteria for aEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause aEDS.
To meet the diagnostic criteria for aEDS, a person must meet:
- Major criterion 1 AND major criterion 3
OR - Major criterion 1 AND major criterion 2 and at least two minor criteria
Major Criteria
- Congenital bilateral hip dislocation
- Severe generalized joint hypermobility, with multiple dislocations/subluxations
- Skin hyperextensibility
Minor Criteria
- Muscle hypotonia
- Kyphoscoliosis
- Radiologically mild osteopenia
- Tissue fragility, including atrophic scars
- Easily bruisable skin
Diagnostic Criteria
To meet the diagnostic criteria for BCS, a person must meet:
Major criterion 1 AND at least one other major criterion
OR
Major criterion 1 AND at least three minor criteria
Major Criteria
- Thin cornea, with or without rupture (central corneal thickness often <400µm)
- Early onset progressive keratoconus
- Early onset progressive keratoglobus
- Blue sclerae
Minor Criteria
- Enucleation or corneal scarring as a result of previous rupture
- Progressive loss of corneal stromal depth, especially in central cornea
- High myopia, with normal or moderately increased axial length
- Retinal detachment
- Deafness, often with mixed conductive and sensorineural components, progressive, higher frequencies often more severely affected (“sloping” pure tone audiogram)
- Hypercompliant tympanic membranes
- Developmental dysplasia of the hip
- Hypotonia in infancy, usually mild if present
- Scoliosis
- Arachnodactyly
- Hypermobility of distal joints
- Pes planus, hallux valgus
- Mild contractures of fingers (especially 5th)
- Soft, velvety skin, translucent skin
Genetic Testing
If a person meets the diagnostic criteria for BCS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause BCS. BCS is caused by having two pathogenic variants in these genes:
- ZNF469
- PRDM5
If a person meets the diagnostic criteria for cvEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause cvEDS.
To meet the diagnostic criteria for cvEDS, a person must meet:
- Major criterion 1 AND family history compatible with autosomal recessive inheritance AND at least one other major criterion
OR - Major criterion 1 AND family history compatible with autosomal recessive inheritance AND at least two minor criteria
Major Criteria
- Severe progressive cardiac-valvular problems (aortic valve, mitral valve)
- Skin involvement: skin hyperextensibility, atrophic scars, thin skin, easy bruising
- Joint hypermobility (generalized or restricted to small joints)
Minor criteria
- Inguinal hernia
- Pectus deformity (especially excavatum)
- Joint dislocations
- Foot deformities: pes planus, pes planovalgus, hallux valgus
If a person meets the diagnostic criteria for clEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause clEDS.
To meet the diagnostic criteria for clEDS, a person must meet all three major criteria AND have a family history compatible with autosomal recessive inheritance.
Major Criteria
- Skin hyperextensibility, with velvety skin texture and absence of atrophic scarring
- Generalized joint hypermobility, with or without recurrent dislocations (most commonly shoulder and ankle)
- Easily bruisable skin/spontaneous ecchymoses
Minor Criteria
- Foot deformities (broad/plump forefoot; brachydactyly with excessive skin; pes planus; hallux valgus; piezogenic papules)
- Edema in the legs in the absence of cardiac failure
- Mild proximal and distal muscle weakness
- Axonal polyneuropathy
- Atrophy of muscles in hands and feet
- Acrogeric hands, mallet finger(s), clinodactyly, brachydactyly
- Vaginal/uterus/rectal prolapse
If a person meets the diagnostic criteria for dEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause dEDS.
To meet the diagnostic criteria for dEDS, a person must meet:
- Major criterion 1 AND major criterion 2 AND at least one other major criterion
OR
- Major criterion 1 AND major criterion 2 AND at least three minor criteria
Major Criteria
- Extreme skin fragility with congenital or postnatal skin tears
- Characteristic craniofacial features, which are evident at birth or early infancy or evolve later in childhood
- Redundant, almost lax skin, with excessive skin folds at the wrists and ankles
- Increased palmar wrinkling
- Severe bruisability with a risk of subcutaneous hematomas and hemorrhage
- Umbilical hernia
- Postnatal growth retardation
- Short limbs, hands, and feet
- Perinatal complications due to connective tissue fragility
Minor Criteria
- Soft and doughy skin texture
- Skin hyperextensibility
- Atrophic scars
- Generalized joint hypermobility
- Complications of visceral fragility (e.g., bladder rupture, diaphragmatic rupture, rectal prolapse)
- Delayed motor development
- Osteopenia
- Hirsutism
- Tooth abnormalities
- Refractive errors (myopia, astigmatism)
- Strabismus
If a person meets the diagnostic criteria for kEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause kEDS.
To meet the diagnostic criteria for kEDS, a person must meet:
- Major criterion 1 AND major criterion 2 AND major criterion 3
OR - Major criterion 1 AND major criterion 2 AND three minor criteria (general or gene-specific)
Major Criteria
- Congenital muscle hypotonia
- Congenital or early onset kyphoscoliosis (progressive or non-progressive)
- Generalized joint hypermobility with dislocations/subluxations (shoulders, hips, and knees in particular)
Minor Criteria
- Skin hyperextensibility
- Easily bruisable skin
- Rupture/aneurysm of a medium-sized artery
- Osteopenia/osteoporosis
- Blue sclerae
- Hernia (umbilical or inguinal)
- Pectus deformity
- Marfanoid habitus
- Talipes equinovarus
- Refractive errors (myopia, hypermetropia)
Gene-Specific Minor Criteria
PLOD1
- Skin fragility (easy bruising, friable skin, poor wound healing, widened atrophic scarring)
- Scleral and ocular fragility/rupture
- Microcornea
- Facial dysmorphology
FKBP14
- Congenital hearing impairment (sensorineural, conductive, or mixed)
- Follicular hyperkeratosis
- Muscle atrophy
- Bladder diverticula
If a person meets the diagnostic criteria for mcEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause mcEDS.
To meet the diagnostic criteria for mcEDS at birth or in early childhood, a person must meet major criterion 1 AND major criterion 2.
To meet the diagnostic criteria for mcEDS in adolescence and adulthood, a person must meet major criterion 1 AND major criterion 3.
Major Criteria
- Congenital multiple contractures, characteristically adduction-flexion contractures and/or talipes equinovarus (clubfoot)
- Characteristic craniofacial features, which are evident at birth or in early infancy
- Characteristic cutaneous features including skin hyperextensibility, easy bruisability, skin fragility with atrophic scars, increased palmar wrinkling
Minor Criteria
- Recurrent/chronic dislocations
- Pectus deformities (flat, excavated)
- Spinal deformities (scoliosis, kyphoscoliosis)
- Peculiar fingers (tapering, slender, cylindrical)
- Progressive talipes deformities (valgus, planus, cavum)
- Large subcutaneous hematomas
- Chronic constipation
- Colonic diverticula
- Pneumothorax/ pneumohemothorax
- Nephrolithiasis/cystolithiasis
- Hydronephrosis
- Cryptorchidism in males
- Strabismus
- Refractive errors (myopia, astigmatism)
- Glaucoma/elevated intraocular pressure
If a person meets the diagnostic criteria for mEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause mEDS.
To meet the diagnostic criteria for mEDS, a person must meet:
- Major criterion 1 AND at least one other major criterion
OR - Major criterion 1 AND at least three minor criteria
Major Criteria
- Congenital muscle hypotonia and/or muscle atrophy that improves with age
- Proximal joint contractures (knee, hip, and elbow)
- Hypermobility of distal joints
Minor Criteria
- Soft, doughy skin
- Atrophic scarring
- Motor developmental delay
- Myopathy on muscle biopsy
If a person meets the diagnostic criteria for pEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause pEDS.
To meet the diagnostic criteria for pEDS, a person must meet:
- Major criterion 1 AND two other major criteria AND one minor criterion
OR - Major criterion 2 AND two other major criteria AND one minor criterion
Major Criteria
- Severe and intractable periodontitis of early onset (childhood or adolescence)
- Lack of attached gingiva
- Pretibial plaques
- Family history of a first-degree relative who meets the clinical diagnostic criteria for pEDS
Minor Criteria
- Easy bruising
- Joint hypermobility, mostly distal joints
- Skin hyperextensibility and fragility, abnormal scarring (wide or atrophic)
- Increased rate of infections
- Hernias
- Marfanoid facial features
- Acrogeria
- Prominent vasculature
If a person meets the diagnostic criteria for spEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause spEDS.
To meet the diagnostic criteria for spEDS, a person must meet major criterion 1 AND major criterion 2 AND have characteristic radiographic abnormalities AND at least two other minor criteria (general or gene-specific).
Major Criteria
- Short stature (progressive in childhood)
- Muscle hypotonia (ranging from severe congenital to mild later onset)
- Bowing of limbs
Minor Criteria
- Skin hyperextensibility, soft, doughy skin, thin, translucent skin
- Pes planus
- Delayed motor development
- Osteopenia
- Delayed cognitive development
Gene-Specific Minor Criteria
B4GALT7
- Radioulnar synostosis
- Bilateral elbow contractures or limited elbow movement
- Generalized joint hypermobility
- Single transverse palmar crease
- Characteristic craniofacial features
- Characteristic radiographic findings
- Severe hypermetropia
- Clouded cornea
B3GALT6
- Kyphoscoliosis (congenital or early onset, progressive)
- Joint hypermobility (generalized or restricted to distal joints, with joint dislocations)
- Joint contractures (congenital or progressive, especially hands)
- Peculiar fingers (slender, tapered, arachnodactyly, spatulate, with broad distal phalanges)
- Talipes equinovarus
- Characteristic craniofacial features
- Tooth discoloration, dysplastic teeth
- Characteristic radiographic findings
- Osteoporosis with multiple spontaneous fractures
- Ascending aortic aneurysm
- Lung hypoplasia, restrictive lung disease
SLC39A13
- Protuberant eyes with bluish sclerae
- Hands with finely wrinkled palms
- Atrophy of the thenar muscles and tapering fingers
- Hypermobility of distal joints
- Characteristic radiologic findings
Diagnostic Criteria
Hypermobile EDS (hEDS)
There is currently no laboratory test available to diagnose hEDS. The diagnosis of hEDS is given to adults who meet the clinical diagnostic criteria for hEDS. Children and adolescents with generalized joint hypermobility can be assessed using the pediatric diagnostic framework.
To meet the diagnostic criteria for hEDS, a person must meet all three criteria (1 and 2 and 3).
Criterion 1: Generalized joint hypermobility
Criterion 2: Two or more of the following features (A, B, and C) must be present
Feature A: Manifestations of a connective tissue disorder (must have five or more of the following):
- Unusually soft or velvety skin
- Mild skin hyperextensibility
- Unexplained striae such as striae distensae or rubrae at the back, groins, thighs, breasts, and/or abdomen in adolescents, men, or pre-pubertal women without a history of significant gain or loss of body fat or weight
- Bilateral piezogenic papules of the heel
- Recurrent or multiple abdominal hernia(s) (e.g., umbilical, inguinal, crural)
- Atrophic scarring involving at least two (2) sites and without the formation of truly papyraceous and/or hemosideric scars as seen in classical EDS
- Pelvic floor, rectal, and/or uterine prolapse in children, men or nulliparous women without a history of morbid obesity or other known predisposing medical condition
- Dental crowding and high or narrow palate
- Arachnodactyly, as defined in one or more of the following:
- positive wrist sign (Steinberg sign) on both sides
- positive thumb sign (Walker sign) on both sides
- Arm span-to-height ratio ≥ 1.05
- Mitral valve prolapse (MVP) mild or greater based on strict echocardiographic criteria
- Aortic root dilatation with Z-score >+2
Feature B: Positive family history (one or more first-degree relatives independently meet the current diagnostic criteria for hEDS)
Feature C: Musculoskeletal complications (must have at least one of the following):
- Musculoskeletal pain in two or more limbs, recurring daily for at least three (3) months
- Chronic, widespread pain for at least three (3) months
- Recurrent joint dislocations or frank joint instability, in the absence of trauma (a or b)
- Three (3) or more atraumatic dislocations in the same joint or two (2) or more atraumatic dislocations in two (2) different joints occurring at different times
OR - Medical confirmation of joint instability at two (2) or more sites not related to trauma
- Three (3) or more atraumatic dislocations in the same joint or two (2) or more atraumatic dislocations in two (2) different joints occurring at different times
Criterion 3: ALL of the following prerequisites must be met:
- Absence of unusual skin fragility, which should prompt consideration of other types of EDS
- Exclusion of other heritable and acquired connective tissue disorders, including autoimmune rheumatologic conditions
- In patients with an acquired connective tissue disorder (e.g., lupus, rheumatoid arthritis, etc.), additional diagnosis of hEDS requires meeting both Features A and B of Criterion 2. Feature C of Criterion 2 (chronic pain and/or instability) cannot be counted towards a diagnosis of hEDS in this situation.
- Exclusion of alternative diagnoses that may also include joint hypermobility by means of hypotonia and/or connective tissue laxity. Alternative diagnoses and diagnostic categories include, but are not limited to:
- Neuromuscular disorders (such as myopathic EDS and Bethlem myopathy)
- Other heritable connective tissue disorders (such as other types of EDS, Loeys–Dietz syndrome, Marfan syndrome)
- Skeletal dysplasias (such as osteogenesis imperfecta)
Classical EDS (cEDS)
If a person meets the diagnostic criteria for cEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has a genetic variant that causes cEDS.
To meet the diagnostic criteria for cEDS, a person must meet:
- Major criterion 1 AND major criterion 2
OR - Major criterion 1 AND three or more minor criteria
Major Criteria
- Skin hyperextensibility and atrophic scarring
- Generalized joint hypermobility
Minor Criteria
- Easy bruising
- Soft, doughy skin
- Skin fragility (or traumatic splitting)
- Molluscoid pseudotumors
- Subcutaneous spheroids
- Hernia (or history thereof)
- Epicanthal folds
- Complications of joint hypermobility (e.g., sprains, dislocations/subluxations, pain, flexible flatfoot)
- Family history of a first-degree relative who meets clinical criteria
- Major criterion 1 AND major criterion 2
Hypermobility Spectrum Disorders (HSD)
HSD in Adults
Adults are diagnosed with HSD if they have symptomatic joint hypermobility that cannot be explained by other conditions. There are four types of HSD in adults based on the type of joint hypermobility present:
HSD in Children and Adolescents
Children and adolescents with generalized joint hypermobility can be assessed using the 2023 Diagnostic Framework for Pediatric Joint Hypermobility. Children with generalized joint hypermobility may fit into one of eight categories based on their symptoms.
Children and adolescents may also be diagnosed with localized HSD (L-HSD) or peripheral HSD (P-HSD) if they have joint hypermobility in specific areas rather than throughout the body. Once a child reaches biological maturity, they can be assessed using the diagnostic criteria for hEDS.
Pediatric Generalized Joint Hypermobility [pGJH] Subtypes: Pediatric generalized joint hypermobility
Musculoskeletal Complications: Absent
Skin and Tissue Abnormalities: Absent
Core Comorbidities: AbsentPediatric Generalized Joint Hypermobility [pGJH] Subtypes: Pediatric generalized joint hypermobility with skin involvement
Musculoskeletal Complications: Absent
Skin and Tissue Abnormalities: Present
Core Comorbidities: AbsentPediatric Generalized Joint Hypermobility [pGJH] Subtypes: Pediatric generalized joint hypermobility with core comorbidities
Musculoskeletal Complications: Absent
Skin and Tissue Abnormalities: Absent
Core Comorbidities: PresentPediatric Generalized Joint Hypermobility [pGJH] Subtypes: Pediatric generalized joint hypermobility with core comorbidities and with skin involvement
Musculoskeletal Complications: Absent
Skin and Tissue Abnormalities: Present
Core Comorbidities: PresentPediatric Generalized Hypermobility Spectrum Disorder [pgHSD] Subtypes: Pediatric generalized hypermobility spectrum disorder, musculoskeletal subtype
Musculoskeletal Complications: Present
Skin and Tissue Abnormalities: Absent
Core Comorbidities: AbsentPediatric Generalized Hypermobility Spectrum Disorder [pgHSD] Subtypes: Pediatric generalized hypermobility spectrum disorder, musculoskeletal subtype with skin involvement
Musculoskeletal Complications: Present
Skin and Tissue Abnormalities: Present
Core Comorbidities: AbsentPediatric Generalized Hypermobility Spectrum Disorder [pgHSD] Subtypes: Pediatric generalized hypermobility spectrum disorder, systemic subtype
Musculoskeletal Complications: Present
Skin and Tissue Abnormalities: Absent
Core Comorbidities: PresentPediatric Generalized Hypermobility Spectrum Disorder [pgHSD] Subtypes: Pediatric generalized hypermobility spectrum disorder, systemic subtype with skin involvement
Musculoskeletal Complications: Present
Skin and Tissue Abnormalities: Present
Core Comorbidities: PresentVascular EDS (vEDS)
Genetic testing is used to see if a person has a genetic variant that causes vEDS. Genetic testing should be considered if a person has any of the major criteria or several minor criteria, particularly in people under the age of 40.
Major Criteria
- Family history of vEDS with a documented causative variant in COL3A1
- Arterial rupture at a young age
- Spontaneous sigmoid colon perforation in the absence of known diverticular disease or other bowel pathology
- Uterine rupture during the third trimester in the absence of previous C-section and/or severe peripartum perineum tears
- Carotid-cavernous sinus fistula (CCSF) formation in the absence of trauma
Minor Criteria
- Bruising unrelated to identified trauma and/or in unusual sites such as the cheeks and back
- Thin, translucent skin with increased venous visibility
- Characteristic facial appearance
- Spontaneous pneumothorax
- Acrogeria
- Talipes equinovarus
- Congenital hip dislocation
- Hypermobility of small joints
- Tendon and muscle rupture
- Keratoconus
- Gingival recession and gingival fragility
- Early-onset varicose veins (under age 30 and starting before pregnancy if female)
Arthrochalasia EDS (aEDS)
If a person meets the diagnostic criteria for aEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause aEDS.
To meet the diagnostic criteria for aEDS, a person must meet:
- Major criterion 1 AND major criterion 3
OR - Major criterion 1 AND major criterion 2 and at least two minor criteria
Major Criteria
- Congenital bilateral hip dislocation
- Severe generalized joint hypermobility, with multiple dislocations/subluxations
- Skin hyperextensibility
Minor Criteria
- Muscle hypotonia
- Kyphoscoliosis
- Radiologically mild osteopenia
- Tissue fragility, including atrophic scars
- Easily bruisable skin
- Major criterion 1 AND major criterion 3
Brittle cornea syndrome (BCS)
Diagnostic Criteria
To meet the diagnostic criteria for BCS, a person must meet:
Major criterion 1 AND at least one other major criterion
ORMajor criterion 1 AND at least three minor criteria
Major Criteria
- Thin cornea, with or without rupture (central corneal thickness often <400µm)
- Early onset progressive keratoconus
- Early onset progressive keratoglobus
- Blue sclerae
Minor Criteria
- Enucleation or corneal scarring as a result of previous rupture
- Progressive loss of corneal stromal depth, especially in central cornea
- High myopia, with normal or moderately increased axial length
- Retinal detachment
- Deafness, often with mixed conductive and sensorineural components, progressive, higher frequencies often more severely affected (“sloping” pure tone audiogram)
- Hypercompliant tympanic membranes
- Developmental dysplasia of the hip
- Hypotonia in infancy, usually mild if present
- Scoliosis
- Arachnodactyly
- Hypermobility of distal joints
- Pes planus, hallux valgus
- Mild contractures of fingers (especially 5th)
- Soft, velvety skin, translucent skin
Genetic Testing
If a person meets the diagnostic criteria for BCS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause BCS. BCS is caused by having two pathogenic variants in these genes:
- ZNF469
- PRDM5
Cardiac-Valvular EDS (cvEDS)
If a person meets the diagnostic criteria for cvEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause cvEDS.
To meet the diagnostic criteria for cvEDS, a person must meet:
- Major criterion 1 AND family history compatible with autosomal recessive inheritance AND at least one other major criterion
OR - Major criterion 1 AND family history compatible with autosomal recessive inheritance AND at least two minor criteria
Major Criteria
- Severe progressive cardiac-valvular problems (aortic valve, mitral valve)
- Skin involvement: skin hyperextensibility, atrophic scars, thin skin, easy bruising
- Joint hypermobility (generalized or restricted to small joints)
Minor criteria
- Inguinal hernia
- Pectus deformity (especially excavatum)
- Joint dislocations
- Foot deformities: pes planus, pes planovalgus, hallux valgus
- Major criterion 1 AND family history compatible with autosomal recessive inheritance AND at least one other major criterion
Classical-like EDS (clEDS)
If a person meets the diagnostic criteria for clEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause clEDS.
To meet the diagnostic criteria for clEDS, a person must meet all three major criteria AND have a family history compatible with autosomal recessive inheritance.
Major Criteria
- Skin hyperextensibility, with velvety skin texture and absence of atrophic scarring
- Generalized joint hypermobility, with or without recurrent dislocations (most commonly shoulder and ankle)
- Easily bruisable skin/spontaneous ecchymoses
Minor Criteria
- Foot deformities (broad/plump forefoot; brachydactyly with excessive skin; pes planus; hallux valgus; piezogenic papules)
- Edema in the legs in the absence of cardiac failure
- Mild proximal and distal muscle weakness
- Axonal polyneuropathy
- Atrophy of muscles in hands and feet
- Acrogeric hands, mallet finger(s), clinodactyly, brachydactyly
- Vaginal/uterus/rectal prolapse
Dermatosparaxis EDS (dEDS)
If a person meets the diagnostic criteria for dEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause dEDS.
To meet the diagnostic criteria for dEDS, a person must meet:
- Major criterion 1 AND major criterion 2 AND at least one other major criterion
OR
- Major criterion 1 AND major criterion 2 AND at least three minor criteria
Major Criteria
- Extreme skin fragility with congenital or postnatal skin tears
- Characteristic craniofacial features, which are evident at birth or early infancy or evolve later in childhood
- Redundant, almost lax skin, with excessive skin folds at the wrists and ankles
- Increased palmar wrinkling
- Severe bruisability with a risk of subcutaneous hematomas and hemorrhage
- Umbilical hernia
- Postnatal growth retardation
- Short limbs, hands, and feet
- Perinatal complications due to connective tissue fragility
Minor Criteria
- Soft and doughy skin texture
- Skin hyperextensibility
- Atrophic scars
- Generalized joint hypermobility
- Complications of visceral fragility (e.g., bladder rupture, diaphragmatic rupture, rectal prolapse)
- Delayed motor development
- Osteopenia
- Hirsutism
- Tooth abnormalities
- Refractive errors (myopia, astigmatism)
- Strabismus
Kyphoscoliotic EDS (kEDS)
If a person meets the diagnostic criteria for kEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause kEDS.
To meet the diagnostic criteria for kEDS, a person must meet:
- Major criterion 1 AND major criterion 2 AND major criterion 3
OR - Major criterion 1 AND major criterion 2 AND three minor criteria (general or gene-specific)
Major Criteria
- Congenital muscle hypotonia
- Congenital or early onset kyphoscoliosis (progressive or non-progressive)
- Generalized joint hypermobility with dislocations/subluxations (shoulders, hips, and knees in particular)
Minor Criteria
- Skin hyperextensibility
- Easily bruisable skin
- Rupture/aneurysm of a medium-sized artery
- Osteopenia/osteoporosis
- Blue sclerae
- Hernia (umbilical or inguinal)
- Pectus deformity
- Marfanoid habitus
- Talipes equinovarus
- Refractive errors (myopia, hypermetropia)
Gene-Specific Minor Criteria
PLOD1
- Skin fragility (easy bruising, friable skin, poor wound healing, widened atrophic scarring)
- Scleral and ocular fragility/rupture
- Microcornea
- Facial dysmorphology
FKBP14
- Congenital hearing impairment (sensorineural, conductive, or mixed)
- Follicular hyperkeratosis
- Muscle atrophy
- Bladder diverticula
- Major criterion 1 AND major criterion 2 AND major criterion 3
Musculocontractural EDS (mcEDS)
If a person meets the diagnostic criteria for mcEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause mcEDS.
To meet the diagnostic criteria for mcEDS at birth or in early childhood, a person must meet major criterion 1 AND major criterion 2.
To meet the diagnostic criteria for mcEDS in adolescence and adulthood, a person must meet major criterion 1 AND major criterion 3.
Major Criteria
- Congenital multiple contractures, characteristically adduction-flexion contractures and/or talipes equinovarus (clubfoot)
- Characteristic craniofacial features, which are evident at birth or in early infancy
- Characteristic cutaneous features including skin hyperextensibility, easy bruisability, skin fragility with atrophic scars, increased palmar wrinkling
Minor Criteria
- Recurrent/chronic dislocations
- Pectus deformities (flat, excavated)
- Spinal deformities (scoliosis, kyphoscoliosis)
- Peculiar fingers (tapering, slender, cylindrical)
- Progressive talipes deformities (valgus, planus, cavum)
- Large subcutaneous hematomas
- Chronic constipation
- Colonic diverticula
- Pneumothorax/ pneumohemothorax
- Nephrolithiasis/cystolithiasis
- Hydronephrosis
- Cryptorchidism in males
- Strabismus
- Refractive errors (myopia, astigmatism)
- Glaucoma/elevated intraocular pressure
Myopathic EDS (mEDS)
If a person meets the diagnostic criteria for mEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause mEDS.
To meet the diagnostic criteria for mEDS, a person must meet:
- Major criterion 1 AND at least one other major criterion
OR - Major criterion 1 AND at least three minor criteria
Major Criteria
- Congenital muscle hypotonia and/or muscle atrophy that improves with age
- Proximal joint contractures (knee, hip, and elbow)
- Hypermobility of distal joints
Minor Criteria
- Soft, doughy skin
- Atrophic scarring
- Motor developmental delay
- Myopathy on muscle biopsy
- Major criterion 1 AND at least one other major criterion
Periodontal EDS (pEDS)
If a person meets the diagnostic criteria for pEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause pEDS.
To meet the diagnostic criteria for pEDS, a person must meet:
- Major criterion 1 AND two other major criteria AND one minor criterion
OR - Major criterion 2 AND two other major criteria AND one minor criterion
Major Criteria
- Severe and intractable periodontitis of early onset (childhood or adolescence)
- Lack of attached gingiva
- Pretibial plaques
- Family history of a first-degree relative who meets the clinical diagnostic criteria for pEDS
Minor Criteria
- Easy bruising
- Joint hypermobility, mostly distal joints
- Skin hyperextensibility and fragility, abnormal scarring (wide or atrophic)
- Increased rate of infections
- Hernias
- Marfanoid facial features
- Acrogeria
- Prominent vasculature
- Major criterion 1 AND two other major criteria AND one minor criterion
Spondylodysplastic EDS (spEDS)
If a person meets the diagnostic criteria for spEDS, genetic testing should be done to confirm the diagnosis. Genetic testing is used to see if a person has the genetic variants that cause spEDS.
To meet the diagnostic criteria for spEDS, a person must meet major criterion 1 AND major criterion 2 AND have characteristic radiographic abnormalities AND at least two other minor criteria (general or gene-specific).
Major Criteria
- Short stature (progressive in childhood)
- Muscle hypotonia (ranging from severe congenital to mild later onset)
- Bowing of limbs
Minor Criteria
- Skin hyperextensibility, soft, doughy skin, thin, translucent skin
- Pes planus
- Delayed motor development
- Osteopenia
- Delayed cognitive development
Gene-Specific Minor Criteria
B4GALT7
- Radioulnar synostosis
- Bilateral elbow contractures or limited elbow movement
- Generalized joint hypermobility
- Single transverse palmar crease
- Characteristic craniofacial features
- Characteristic radiographic findings
- Severe hypermetropia
- Clouded cornea
B3GALT6
- Kyphoscoliosis (congenital or early onset, progressive)
- Joint hypermobility (generalized or restricted to distal joints, with joint dislocations)
- Joint contractures (congenital or progressive, especially hands)
- Peculiar fingers (slender, tapered, arachnodactyly, spatulate, with broad distal phalanges)
- Talipes equinovarus
- Characteristic craniofacial features
- Tooth discoloration, dysplastic teeth
- Characteristic radiographic findings
- Osteoporosis with multiple spontaneous fractures
- Ascending aortic aneurysm
- Lung hypoplasia, restrictive lung disease
SLC39A13
- Protuberant eyes with bluish sclerae
- Hands with finely wrinkled palms
- Atrophy of the thenar muscles and tapering fingers
- Hypermobility of distal joints
- Characteristic radiologic findings
FAQs
What features suggest a person might have a type of EDS or HSD?
Each type of EDS has a different set of features that distinguish it from other types. Some features can occur in every type, including joint hypermobility, skin hyperextensibility, and tissue fragility.
EDS may be suspected if a person has these features, but many other conditions share features with EDS. It is important to rule out these other conditions because they may be managed differently. If a person has symptomatic joint hypermobility that cannot be explained by any type of EDS or other conditions, then the hypermobility spectrum disorders may be considered.
How can you tell the difference between different types of EDS?
Some features can be seen across many types of EDS, but each condition has a unique set of features that distinguishes it from other types. These differences are reflected in the diagnostic criteria for each type of EDS. If a person meets the diagnostic criteria for a type of EDS, genetic testing should be done to confirm the diagnosis.
Genetic testing is not available for hEDS, so people with hEDS do not need genetic testing unless there is reason to suspect they may have another type of EDS or another genetic disorder.
Type of EDS Distinguishing Features Hypermobile EDS (hEDS) Generalized joint hypermobility Joint instability
Chronic pain
Classical EDS (cEDS) Skin fragility with extensive atrophic scarring Very stretchy skin with a velvety or doughy texture
Vascular EDS (vEDS) Arterial fragility with aneurysm/dissection/rupture Organ fragility and rupture
Extensive bruising
Pneumothorax (collapsed lung)
Periodontal EDS (pEDS) Severe, early-onset gum disease with tooth loss Pretibial plaques (discoloration of shins)
Kyphoscoliotic EDS (kEDS) Congenital/early-onset kyphoscoliosis Congenital hypotonia (low muscle tone)
Spondylodysplastic EDS (spEDS) Short stature Muscle weakness
Limb bowing
Craniofacial features
Brittle cornea syndrome (BCS) Severe problems with the cornea of the eye Hearing loss
Arthrochalasia EDS (aEDS) Severe joint hypermobility Congenital bilateral hip dislocation
Musculocontractural EDS (mcEDS) Congenital multiple contractures Craniofacial features
Classical-like EDS (clEDS) Stretchy, velvety skin without atrophic scarring Foot deformities
Leg swelling
Dermatosparaxis EDS (dEDS) Severe skin fragility Craniofacial features
Loose, excess skin
Severe bruising
Short limbs
Myopathic EDS (mEDS) Congenital hypotonia (low muscle tone at birth) Proximal joint contractures
Cardiac-valvular EDS (cvEDS) Severe heart valve insufficiency How is joint hypermobility assessed?
Joint hypermobility means the joints have a greater range of motion than is expected or normal. A doctor or physical therapist can evaluate a person’s joints to determine if they are hypermobile. For some joints, a tool called a goniometer can be used to measure how far the joint can extend. People may have joint hypermobility in one, a few, or many of their joints. Joint hypermobility is classified by which joints are affected.
- Generalized joint hypermobility: joint hypermobility present in many different joints throughout the body
- Peripheral joint hypermobility: joint hypermobility limited to the hands and feet
- Localized joint hypermobility: joint hypermobility in a single joint or group of joints in the same area
The Beighton Score is a screening tool for generalized joint hypermobility that measures joint hypermobility on a 9-point scale.
How is skin hyperextensibility measured?
Skin extensibility, or skin stretchiness, is measured by pinching and gently pulling the skin to measure the distance it can stretch. At this time, the doctor can also examine the thickness and texture of the skin. Skin extensibility is usually measured on the ventral (underside) of the forearm, the back of the hand, or the neck.
Skin is hyperextensible if it stretches greater than:
- 1.5 cm on the forearms
- 1.5 cm on the back of the hands
- 3 cm on the neck
- 3 cm on the knees
Mild skin hyperextensibility may occur in people with any type of EDS. More severe skin hyperextensibility is observed in certain types of EDS.
What conditions must be ruled out for someone to be diagnosed with hEDS or HSD?
No lab test or imaging study can prove that someone does or does not have hEDS or HSD. Other explanations for a person’s symptoms must be ruled out before they can be diagnosed with hEDS or HSD. Other conditions can often be ruled out based on a person’s symptoms and family history. Testing is not needed to rule out other conditions unless there is reason to suspect that a person may have a different condition.
Conditions that should be ruled out include:
- The other types of Ehlers-Danlos syndrome
- Other heritable connective tissue disorders such as Marfan syndrome, Loeys-Dietz syndrome, and Stickler syndrome
- Skeletal dysplasias such as osteogenesis imperfecta
- Autoimmune rheumatic connective tissue disorders such as lupus and rheumatoid arthritis
- Chromosomal conditions such as Fragile X syndrome, Kabuki syndrome, and Down syndrome
- Neuromuscular disorders that can cause joints to become unstable, such as multiple sclerosis and myopathies
If these conditions are present but do not explain the person’s symptoms, then hEDS or HSD may also be present. In addition to ruling out the conditions above, adults can only be diagnosed with HSD if they do not meet the diagnostic criteria for hEDS.
What types of doctors can diagnose EDS and HSD?
To be assessed for a type of EDS, it is best to see a doctor who has experience with heritable connective tissue disorders. This may be a geneticist, rheumatologist, or another type of doctor, depending on where you live and the type of EDS you may have.
There is no lab test for hEDS or HSD, so these conditions are diagnosed based on medical history, physical examination, and by ruling out other conditions. Any doctor can diagnose hEDS and HSD if they have enough experience to apply the diagnostic criteria and feel comfortable ruling out alternative diagnoses.
What are diagnostic criteria?
Clinical diagnostic criteria are a set of signs, symptoms, and tests that can be used to make a diagnosis. Each type of EDS has its own diagnostic criteria that describe the set of features associated with that type. The diagnostic criteria define what is required for a person to be diagnosed with each type of EDS.
Genetic testing is used to confirm the diagnosis of some types of EDS. Genetic testing is not available for hEDS, so hEDS is diagnosed based on signs, symptoms, and family history.
What if a person meets the clinical diagnostic criteria but does not have positive genetic testing results?
Sometimes, a “provisional clinical diagnosis” of a type of EDS is made without positive genetic testing results. This may happen when a person meets the clinical diagnostic criteria for a type of EDS but does not have access to genetic testing. This can also happen when a person meets the clinical diagnostic criteria but genetic testing is negative or shows a variant of uncertain significance. In these cases, the person’s symptoms should be clearly distinguishable from other conditions, including other types of EDS. Some symptoms are common across most types of EDS, such as joint hypermobility, pain, and fatigue. A provisional clinical diagnosis should only be made when no alternative diagnoses can be made to explain a person’s symptoms.
What types of tests are used to diagnose EDS?
Next-generation sequencing (NGS) is the most common approach for diagnosing most types of EDS. NGS can be used to identify the genetic variants a person has for specific gene(s) of interest.
Targeted sequencing can be used to look at a single gene or a group of genes, known as a gene panel. Some labs offer an “Ehlers-Danlos syndrome panel” or “connective tissue disorder panel” that includes many of the genes known to cause types of EDS and other heritable connective tissue disorders. Doctors can also request to test specific genes based on a person’s signs and symptoms.
Whole genome sequencing (WGS) is used to look at all of a person’s DNA. Whole exome sequencing (WES) can be used to look at all the DNA expressed in the body. These tests are often used for research, such as identifying new pathogenic genetic variants. Single gene tests and gene panels provide a much more targeted approach when looking for specific genetic variants in genes of interest.
If sequencing does not identify pathogenic variants, a copy number variant (CNV) detection strategy can be used to identify large duplications and deletions.
If genetic testing is not available, other techniques can be used to detect differences in proteins that occur in certain types of EDS. These tests include SDS-PAGE and HPLC.
FAQs
What features suggest a person might have a type of EDS or HSD?
Each type of EDS has a different set of features that distinguish it from other types. Some features can occur in every type, including joint hypermobility, skin hyperextensibility, and tissue fragility.
EDS may be suspected if a person has these features, but many other conditions share features with EDS. It is important to rule out these other conditions because they may be managed differently. If a person has symptomatic joint hypermobility that cannot be explained by any type of EDS or other conditions, then the hypermobility spectrum disorders may be considered.
How can you tell the difference between different types of EDS?
Some features can be seen across many types of EDS, but each condition has a unique set of features that distinguishes it from other types. These differences are reflected in the diagnostic criteria for each type of EDS. If a person meets the diagnostic criteria for a type of EDS, genetic testing should be done to confirm the diagnosis.
Genetic testing is not available for hEDS, so people with hEDS do not need genetic testing unless there is reason to suspect they may have another type of EDS or another genetic disorder.
Type of EDS: Hypermobile EDS (hEDS)
Distinguishing Features:
Generalized joint hypermobility
Joint instability
Chronic painType of EDS: Classical EDS (cEDS)
Distinguishing Features:
Skin fragility with extensive atrophic scarring
Very stretchy skin with a velvety or doughy textureType of EDS: Vascular EDS (vEDS)
Distinguishing Features:
Arterial fragility with aneurysm/dissection/rupture
Organ fragility and rupture
Extensive bruising
Pneumothorax (collapsed lung)Type of EDS: Periodontal EDS (pEDS)
Distinguishing Features:
Severe, early-onset gum disease with tooth loss
Pretibial plaques (discoloration of shins)Type of EDS: Kyphoscoliotic EDS (kEDS)
Distinguishing Features:
Congenital/early-onset kyphoscoliosis
Congenital hypotonia (low muscle tone)Type of EDS: Spondylodysplastic EDS (spEDS)
Distinguishing Features:
Short stature
Muscle weakness
Limb bowing
Craniofacial featuresType of EDS: Brittle cornea syndrome (BCS)
Distinguishing Features:
Severe problems with the cornea of the eye
Hearing lossType of EDS: Arthrochalasia EDS (aEDS)
Distinguishing Features:
Severe joint hypermobility
Congenital bilateral hip dislocationType of EDS: Musculocontractural EDS (mcEDS)
Distinguishing Features:
Congenital multiple contractures
Craniofacial featuresType of EDS: Classical-like EDS (clEDS)
Distinguishing Features:
Stretchy, velvety skin without atrophic scarring
Foot deformities
Leg swellingType of EDS: Dermatosparaxis EDS (dEDS)
Distinguishing Features:
Severe skin fragility
Craniofacial features
Loose, excess skin
Severe bruising
Short limbsType of EDS: Myopathic EDS (mEDS)
Distinguishing Features:
Congenital hypotonia (low muscle tone at birth)
Proximal joint contracturesType of EDS: Cardiac-valvular EDS (cvEDS)
Distinguishing Features:
Severe heart valve insufficiencyHow is joint hypermobility assessed?
Joint hypermobility means the joints have a greater range of motion than is expected or normal. A doctor or physical therapist can evaluate a person’s joints to determine if they are hypermobile. For some joints, a tool called a goniometer can be used to measure how far the joint can extend. People may have joint hypermobility in one, a few, or many of their joints. Joint hypermobility is classified by which joints are affected.
- Generalized joint hypermobility: joint hypermobility present in many different joints throughout the body
- Peripheral joint hypermobility: joint hypermobility limited to the hands and feet
- Localized joint hypermobility: joint hypermobility in a single joint or group of joints in the same area
The Beighton Score is a screening tool for generalized joint hypermobility that measures joint hypermobility on a 9-point scale.
How is skin hyperextensibility measured?
Skin extensibility, or skin stretchiness, is measured by pinching and gently pulling the skin to measure the distance it can stretch. At this time, the doctor can also examine the thickness and texture of the skin. Skin extensibility is usually measured on the ventral (underside) of the forearm, the back of the hand, or the neck.
Skin is hyperextensible if it stretches greater than:
- 1.5 cm on the forearms
- 1.5 cm on the back of the hands
- 3 cm on the neck
- 3 cm on the knees
Mild skin hyperextensibility may occur in people with any type of EDS. More severe skin hyperextensibility is observed in certain types of EDS.
What conditions must be ruled out for someone to be diagnosed with hEDS or HSD?
No lab test or imaging study can prove that someone does or does not have hEDS or HSD. Other explanations for a person’s symptoms must be ruled out before they can be diagnosed with hEDS or HSD. Other conditions can often be ruled out based on a person’s symptoms and family history. Testing is not needed to rule out other conditions unless there is reason to suspect that a person may have a different condition.
Conditions that should be ruled out include:
- The other types of Ehlers-Danlos syndrome
- Other heritable connective tissue disorders such as Marfan syndrome, Loeys-Dietz syndrome, and Stickler syndrome
- Skeletal dysplasias such as osteogenesis imperfecta
- Autoimmune rheumatic connective tissue disorders such as lupus and rheumatoid arthritis
- Chromosomal conditions such as Fragile X syndrome, Kabuki syndrome, and Down syndrome
- Neuromuscular disorders that can cause joints to become unstable, such as multiple sclerosis and myopathies
If these conditions are present but do not explain the person’s symptoms, then hEDS or HSD may also be present. In addition to ruling out the conditions above, adults can only be diagnosed with HSD if they do not meet the diagnostic criteria for hEDS.
What types of doctors can diagnose EDS and HSD?
To be assessed for a type of EDS, it is best to see a doctor who has experience with heritable connective tissue disorders. This may be a geneticist, rheumatologist, or another type of doctor, depending on where you live and the type of EDS you may have.
There is no lab test for hEDS or HSD, so these conditions are diagnosed based on medical history, physical examination, and by ruling out other conditions. Any doctor can diagnose hEDS and HSD if they have enough experience to apply the diagnostic criteria and feel comfortable ruling out alternative diagnoses.
What are diagnostic criteria?
Clinical diagnostic criteria are a set of signs, symptoms, and tests that can be used to make a diagnosis. Each type of EDS has its own diagnostic criteria that describe the set of features associated with that type. The diagnostic criteria define what is required for a person to be diagnosed with each type of EDS.
Genetic testing is used to confirm the diagnosis of some types of EDS. Genetic testing is not available for hEDS, so hEDS is diagnosed based on signs, symptoms, and family history.
What if a person meets the clinical diagnostic criteria but does not have positive genetic testing results?
Sometimes, a “provisional clinical diagnosis” of a type of EDS is made without positive genetic testing results. This may happen when a person meets the clinical diagnostic criteria for a type of EDS but does not have access to genetic testing. This can also happen when a person meets the clinical diagnostic criteria but genetic testing is negative or shows a variant of uncertain significance. In these cases, the person’s symptoms should be clearly distinguishable from other conditions, including other types of EDS. Some symptoms are common across most types of EDS, such as joint hypermobility, pain, and fatigue. A provisional clinical diagnosis should only be made when no alternative diagnoses can be made to explain a person’s symptoms.
What types of tests are used to diagnose EDS?
Next-generation sequencing (NGS) is the most common approach for diagnosing most types of EDS. NGS can be used to identify the genetic variants a person has for specific gene(s) of interest.
Targeted sequencing can be used to look at a single gene or a group of genes, known as a gene panel. Some labs offer an “Ehlers-Danlos syndrome panel” or “connective tissue disorder panel” that includes many of the genes known to cause types of EDS and other heritable connective tissue disorders. Doctors can also request to test specific genes based on a person’s signs and symptoms.
Whole genome sequencing (WGS) is used to look at all of a person’s DNA. Whole exome sequencing (WES) can be used to look at all the DNA expressed in the body. These tests are often used for research, such as identifying new pathogenic genetic variants. Single gene tests and gene panels provide a much more targeted approach when looking for specific genetic variants in genes of interest.
If sequencing does not identify pathogenic variants, a copy number variant (CNV) detection strategy can be used to identify large duplications and deletions.
If genetic testing is not available, other techniques can be used to detect differences in proteins that occur in certain types of EDS. These tests include SDS-PAGE and HPLC.