
Updated: January 9, 2023
EDS & HSD and COVID-19

What Health Conditions Increase the Risk of Complications from COVID-19 in the General Population?
Some individuals in the general population are described as having a higher risk for complications of covid-19 compared to others. The World Health Organization [WHO], Center for Disease Control and Prevention [CDC], and other official groups have said these are:
- The Elderly
- People with a pre-existing heart condition
- People with high blood pressure
- Diabetes
- The presence of any underlying lung condition
- Reduced immunity, which would include medications for autoimmune diseases
NHS England provides a list of conditions within the above categories that are considered to be particularly ‘High’ risk, or ‘Very High’ risk. These can be found here.
How Do These Risks Apply to a Person with EDS or HSD?
For a person with EDS or HSD the risk of getting complications from covid-19 will depend on the nature of that persons’ specific health concerns. Some people may have one or more of the risks listed. But many people with EDS or HSD will not have these risk factors.
Thinking about the risk factors for complications:
This might include heart valve disease (moderate to severe valve disease), aneurysms/dissections (VASCERN, Vascular Disease Network), and severe pectus deformity that has caused changes in heart function.
It is not known if mild mitral valve prolapse (MVP) is a particular risk for complications from COVID-19 infection.
Rarely, bacteria that enter the bloodstream can cause a condition called endocarditis, an infection of the inner lining of the heart chambers and valves. This risk is higher in people with Mitral Valve Prolapse because the deformed mitral valve flap can attract bacteria that are in the bloodstream.
Postural Orthostatic Tachycardia Syndrome (POTS) is not known to be a risk but may worsen because of dehydration if unwell.
There are many causes of lung disease that are not known to be related to having EDS or HSD. However, there are lung conditions that arise in EDS that should be considered:
- One concern may be poor lung volumes that can occur if a person has severe kyphosis/scoliosis, or emphysema, that might increase the risk of pneumonia.
- In addition, persistent dry cough and sudden/increasing shortness of breath could arise from a pneumothorax (sudden partial or complete collapse of a lung). A pneumothorax can be spontaneous or may arise in a person known to have cystic (bullous) lung disease. Forceful coughing from a respiratory infection may cause a pneumothorax but there is no way to know if this is a particular risk in an individual unless they have had a pneumothorax before.
- Also, some individuals with EDS and HSD have apnea (breathing stops and starts, especially when sleeping) (Sedky K et al. J Clin Sleep Med. 2019 Feb 15;15(2):293-299. Meta-analysis). If you have this, it should be raised with an attending doctor if you are experiencing worsening breathing symptoms.
- Symptoms of wheeze and cough are common in EDS – affecting on average 15-20% of hEDS, cEDS and vEDS individuals in a recent large survey (Sheehan TP et al. Respiratory Symptoms Among Patients with Ehlers-Danlos Syndromes (eds). ATS Conferences. 2017; C37). With regard to COVID-19, and any other respiratory infections, the change in the severity of these symptoms should be alerted to an attending doctor if a person is concerned that they are developing a respiratory infection.
The immune system is suppressed by medications such as steroids, and disease-modifying drugs like azathioprine, methotrexate.
In Mast Cell Activation Syndrome (MCAS) reports suggest that medications used to treat the condition may be helpful in people with COVID-19 infection. (Forster-Ruhrman et al. (May 2020), Afrin et al. (September 2020)). Afrin et al. report that none of their treated MCAS patient who have had COVID-19 have experienced the severe complications that can arise from the infection.
Also, a practitioners guide to the assessment and management of individuals with MCAS in light of COVID-19 has been published. (Valent et al. (August 2020). The authors of the guide state that they hope that their advice will reduce fears among MCAS patients. They conclude that as more data becomes available regarding the consequences of COVID-19 infection in people with MCAS, more specific recommendations with higher levels of evidence will be produced.
Other Specific Concerns That People with EDS or HSD Might Have
Postural Orthostatic Tachycardia Syndrome (POTS) and Orthostatic Hypotension (OH) are not known to be risks for developing greater complications from COVID-19. However, symptoms of POTS or OH may worsen if a person becomes very dehydrated with any illness, including COVID-19. The advice is to try and maintain good fluid intake.
Dysautonomia International discusses the impact of COVID-19 in a webinar that can be found here.
Some may be concerned because they are pregnant. The Royal College of Obstetrics and Gynaecology, UK has given this opinion:
“Generally, pregnant women do not appear to be more likely to be seriously unwell than other healthy adults if they develop the new coronavirus. It is expected the large majority of pregnant women will experience only mild or moderate cold/flu like symptoms” (RCOG, 9 April 2020).
An article in the New Scientist (March 16 2020) said:
“One reason to worry about covid-19 in pregnancy is that people are more likely to become severely ill with flu when they are pregnant…However, initial reports suggest that covid-19 might not hit pregnant women or their newborn babies too heavily.”
In the UK the Government has today (March 17, 2020) included pregnancy as a risk and advised that people self-isolate for 12 weeks like others at risk. Information and links are on the BBC website.
There has been advice in the media very recently that Ibuprofen (an Non-Steroidal Anti Inflammatory Drug, or NSAID) should be avoided for symptom relief from covid-19. Studies suggest ibuprofen can dampen down the immune system and slow recovery from infection. When taken during an infection Ibuprofen may cause more severe illness and complications. The advice is to use paracetamol instead.
In an NHS England statement, March 17, 2020 the advice given is that those currently on NSAIDs for other medical reasons (e.g. arthritis) should not stop them. The WHO also states (March 19, 2020) that they are not aware of any reports that ibuprofen causes the illness from covid-19 infection to be more severe.
The European Medicines Agency (EMA, 18 March 2020) has said “There is currently no scientific evidence establishing a link between ibuprofen and worsening of COVID‑19”. This has been further affirmed by the MHRA (14 April 2020).
The Renin-Angiotensin Aldosterone System (RAAS) inhibitors include the following medications:
- ACE inhibitors – Enalapril, lisinopril, ramipril, captopril, benazepril
- ARBs – Valsartan, candesartan, losartan, irbesartan
- Direct renin inhibitors – Aliskiren
Researchers have concluded that there is no increased risk of complications from COVID-19 from taking a RAAS Inhibitor medication. A scientific review (Tignanelli and colleagues, March 2020) in The Lancet Respiratory Medicine, and in a study in the New England Journal of Medicine (NEJM) Reynolds and colleagues (May 2020) has looked at these concerns. A lay summary of the findings by Reynolds is discussed in a New York Times article. In addition, in the NEJM Mehra and colleagues report similar conclusions to Reynolds. Also, later in May 2020 Ackermann and colleagues report similar observations regarding vascular concerns in the lungs. These findings suggest that statins (lipid lowering drugs) and RAAS medications may protect against the vascular damage seen in severe COVID-19 disease. Clinical trials are needed to confirm this.
Kawasaki disease (KD) is rare. In North America and Europe, it affects around 8-20 per 100,000 children (typically children under the age of five years old). In Northeast Asian countries such as Japan it is much more prevalent.
The cause of Kawasaki disease is unknown. It appears to be triggered by infection, but it is also thought to be triggered in some cases by an autoimmune process, or an ‘autoinflammatory’ process (a process that does not involve infection or autoimmune pathways).
One major complication of KD is spontaneous coronary artery dissection (SCAD). A study over 11 years of over 65,000 patients with SCAD found that 10 people had Marfan syndrome, and 10 had Ehlers-Danlos syndrome. The small numbers of cases of EDS make it hard to reach any conclusions about associations between these conditions.
The scientific literature and News are reporting that children with COVID-19 infection are falling severely ill with a toxic shock-like reaction described as similar to Kawasaki disease. Source 1. Source 2.
Dr. Jane Newburger Director of the Kawasaki Program at Boston Children’s Hospital; and Commonwealth Professor of Pediatrics at Harvard Medical School, in an article for The American Heart Association said: “We want to reassure parents – this appears to be uncommon. While Kawasaki disease can damage the heart or blood vessels, the heart problems usually go away in five or six weeks, and most children fully recover. Rarely, but sometimes, the coronary artery damage persists. Because of this, Kawasaki disease is the most common cause of acquired heart disease in children in developed countries. Prompt treatment is critical to prevent significant heart problems.”
At this time there is no evidence that specific greater complications from Kawasaki-like disease arise in children with EDS or HSD. The Ehlers-Danlos Society’s message to our community remains that, as for all other diseases and health concerns, it is essential that doctors assessing or treating a child with EDS or HSD for COVID-19 and its complications know that the child has EDS or HSD, all the complications from their EDS or HSD, and all the treatments they are on.
Antibiotics do not kill viruses, but a person with a viral infection may develop an added bacterial infection. First-line antibiotics for bacterial pneumonia include: Penicillin (e.g. Amoxicillin); a Macrolide (e.g. Clarithromycin); and Tetracyclines (e.g. Doxycycline). Second line might include Fluoroquinolones (e.g. Ciprofloxacin / Levofloxacin / Norfloxacin).
The FDA, EMA, and other international medicines regulator guidance indicate that patients who have an aortic aneurysm or are at risk of an aortic aneurysm should not be prescribed fluoroquinolones unless no other suitable treatment is available.
In the Ehlers-Danlos syndromes this risk applies primarily to vascular Ehlers-Danlos syndrome [vEDS]. Sometimes individuals with other rare types of EDS may also have aortic aneurysms, or any person may have an aneurysm for another reason – the guidance applies to these people too.
Most people with EDS (with the exception of the groups listed above) are not at increased risk of an aneurysm from their EDS.
In addition, the FDA, MHRA, and other international medicines regulators have published that, rarely, fluoroquinolones can cause serious and potentially irreversible complications that affect tendons, muscles, joints, nerves, and the central nervous system. There have been cases, for example, where tendon inflammation and tendon rupture has occurred. Notably (but not exclusively) this has occurred at the Achilles tendon. The increased risks of tendon rupture appear to be aged 60 years and over and taking corticosteroids at the same time as taking the fluoroquinolone. Research suggests that ofloxacin and norfloxacin have the greatest risk for tendon rupture (Alves et al Eur J Clin Pharmacol 2019;75:1431-1443 Meta-analysis).
The specific risk of tendon rupture and other non-vascular side effects in EDS or HSD, compared to the general population, is not known.
To reduce risk in the general population the guidance states that fluoroquinolones should not be used for uncomplicated infections (e.g. mild-moderate sinusitis, bronchitis, or cystitis) unless there is no other suitable class of antibiotic.
A fluoroquinolone may be the only suitable antibiotic to fight an infection because, for example, bacteria are resistant to other types of antibiotic, or the infection is causing serious complications such as sepsis. In these situations, doctors with their patients have to determine whether the benefits of taking a fluoroquinolone outweigh the risks.
The following is taken from The American College of Gastroenterology, March 16, 2020. It applies to everyone but some people with EDS or HSD have issues with bowel function and should maintain good hygiene.
- There is evidence suggesting that Coronavirus could be spread from feces.
- Cough, fever, fatigue, or sore throat are the most common symptoms in adults
- But GI symptoms including nausea and/or diarrhea may also occur in some cases.
- The virus may be present in GI mucous secretions and feces.
- Gastrointestinal infection and the potential to pass on infection from fecal contamination / poor hand hygiene must be considered like any other diarrheal illness.
Long COVID or Long Haul COVID is the term used to describe the long-term ill-health that can arise after contracting COVID-19. It is a complex post-infection syndrome. The development of symptoms after an infection is not a new phenomenon. ‘Post-viral fatigue’ for example is a recognized disorder. The chronic symptoms and significant functional impairment of ME/CFS may be triggered or worsened by infection. However, awareness of this has dramatically increased, likely because Long COVID is affecting so many people.
Carfi A et al. (2020) published one of the first studies on the longer-term effects of COVID-19 infection. In 143 patients hospitalized with COVID-19 infection, the study found that 32% continued to experience one or two symptoms 60 days after the onset of COVID-19, and 55% had three or more symptoms. These symptoms included fatigue (53%), difficulty in breathing (43%), joint pain (27%), and chest pain (22%). The study found a worsened quality of life in 44% of patients. Others, such as the large international study by Davis et al. (2021), have found similar results and reported an extensive list of Long COVID symptoms.
However, before COVID-19 ever appeared, many people in the HSD, EDS, ME/CFS, and Mast Cell Activation Diseases communities already had concerns that are now also described in Long COVID. For example, a survey of the Ehlers-Danlos Society Global Registry showed (from 1340 responses and prior to COVID-19’s appearance) that 98% of those with HSD or EDS surveyed had joint pain and chronic fatigue and 74% had breathing difficulties. Other common concerns include POTS and MCAD.
One of the challenges now is knowing whether new or worsening symptoms are due to concerns already seen in conditions like HSD or EDS, or due to catching COVID-19, or due to both compounding each other. Either way, we hope the clinics and research set up to support people with Long COVID will help generally in advancing the understanding and treatment of these chronic symptoms.
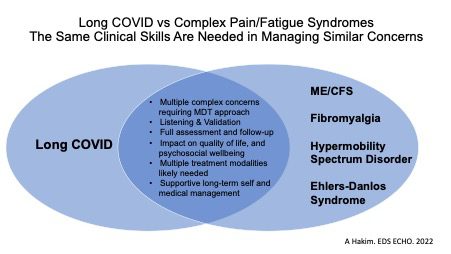
Depicted in the first of the two diagrams below, we believe there are important transferable skills between the clinics and clinicians assessing and caring for people with all these chronic and complex conditions, whether a person is seen for Long COVID or EDS/HSD or both.
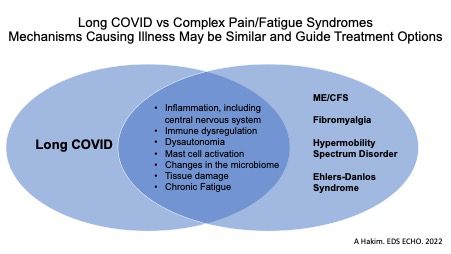
The second diagram shows the mechanisms and common conditions shared between Long COVID and EDS/HSD and other conditions.
In addition, we are aware of recent findings in the scientific literature that suggest COVID-19 infection and/or reactions to COVID-19 vaccinations may have a variety of effects on the extracellular matrix. This gives intriguing insights into aspects of collagen and matrix biology that may be relevant to further understanding EDS, HSD, and other connective tissue disorders. However, currently there is no clear evidence that COVID-19 infection causes EDS or HSD.
We continue to work closely with our academic and clinical experts, other charities and coalitions working in this area, and the EDS and HSD community to understand all the implications of COVID-19.
We are aware of the latest news regarding two people with histories of severe allergy in the UK having an allergic reaction to the Pfizer BioNTech vaccination for COVID-19.
A number of our community have allergies and intolerances to medicines. Those with a history of severe reactions, for example needing to carry an adrenaline autoinjector to treat anaphylaxis, should follow the MHRA advice or discuss their concerns with their doctor.
The MHRA has issued the following advice: “Any person with a history of anaphylaxis to a vaccine, medicine or food should not receive the Pfizer/BioNTech vaccine.”
The Ehlers-Danlos Society has received a number of enquiries as to whether people with EDS or HSD should have a COVID-19 vaccination. We are not aware of any studies that have looked specifically at EDS or HSD. Many with EDS or HSD have chronic and complex health concerns that potentially could worsen with COVID-19 infection. For the majority of our community, like so many others with chronic illnesses, the benefits of protection against the COVID-19 virus are likely to out-weigh the risks associated with having the infection (including Long Covid) or getting side-effects of the vaccination.
That said, an individual with EDS or HSD may have a history of severe reactions to injections such as the flu jab or pneumococcal vaccine, or they may have a history of anaphylaxis. In these situations, or if there are specific health concerns, individuals should discuss the risks of having a COVID-19 vaccination with their attending doctor.
The Society has also been asked about protein-based vaccines versus mRNA vaccines. A lay summary of how vaccines work can be found on the CDCs website here.
A summary of what mRNA vaccines are is available here.
In addition, the CDC has produced general advice for Clinicians that is available here.
As European Reference Networks (ERNs) are formed by experts in rare diseases, all ERNs provided their opinions on the priorities and contraindications for patients with a rare disease within their network. The results are summarized in this document and were discussed during the internal ERN-Coordinator group meeting of January 27, 2021.
Regularly and thoroughly clean your hands with an alcohol-based hand rub or wash them with soap and water.
Why? Washing your hands with soap and water or using alcohol-based hand rub kills viruses that may be on your hands.
When in public spaces maintain at least 2 meter distance between you and other people who are not members of your household.
Why? When someone coughs or sneezes they spray small liquid droplets from their nose or mouth which may contain virus. If you are too close, you can breathe in the droplets, including the COVID-19 virus if the person coughing has the disease.
Why? Hands touch many surfaces and can pick up viruses. Once contaminated, hands can transfer the virus to your eyes, nose or mouth. From there, the virus can enter your body and can make you sick.
Make sure you, and the people around you, follow good respiratory hygiene. This means covering your mouth and nose with your bent elbow or tissue when you cough or sneeze. Then dispose of the used tissue immediately.
Why? Droplets spread virus. By following good respiratory hygiene you protect the people around you from viruses such as cold, flu and COVID-19.
Stay at home if you begin to feel unwell, even with mild symptoms such as headache and slight runny nose, until you recover.
If you have a fever, cough and difficulty breathing, seek medical attention and call in advance. Follow the directions of your local health authority.
Why? National and local authorities will have the most up to date information on the situation in your area. Calling in advance will allow your health care provider to quickly direct you to the right health facility. This will also protect you and help prevent spread of viruses and other infections.
Stay informed on the latest developments about COVID-19. Follow advice given by your healthcare provider, your national and local public health authority or your employer on how to protect yourself and others from COVID-19.
Why? National and local authorities will have the most up to date information on whether COVID-19 is spreading in your area. They are best placed to advise on what people in your area should be doing to protect themselves.